Stem Cell Therapy for Facet Syndrome
Stem Cell Therapy for Facet Syndrome
Stem cell therapy for facet syndrome reduces pain, decreases inflammation, and increases spinal mobility by regenerating damaged joint tissue. Long-term recovery with Stemcell Consultancy.
Picture this: a 54-year-old engineer who hasn't slept through the night in two years. Not because of stress or a screen addiction — but because turning over in bed sends a sharp, grinding pain from his lower back down into his buttocks. He's had the X-rays, the MRI, the nerve block injections. He's been told his spine "looks like it belongs to someone older." He's tried three different pain management regimens and two rounds of physical therapy. Every morning, he gets out of bed the same way: slowly, carefully, bracing for the first wave of stiffness that takes thirty minutes to ease.
His diagnosis? Facet joint syndrome. His situation? Shared by an estimated 15 to 45 percent of all chronic low back pain patients — making it one of the most common, and most consistently overlooked, sources of spinal pain worldwide.
This is the story of what's changing.
Understanding Facet Syndrome
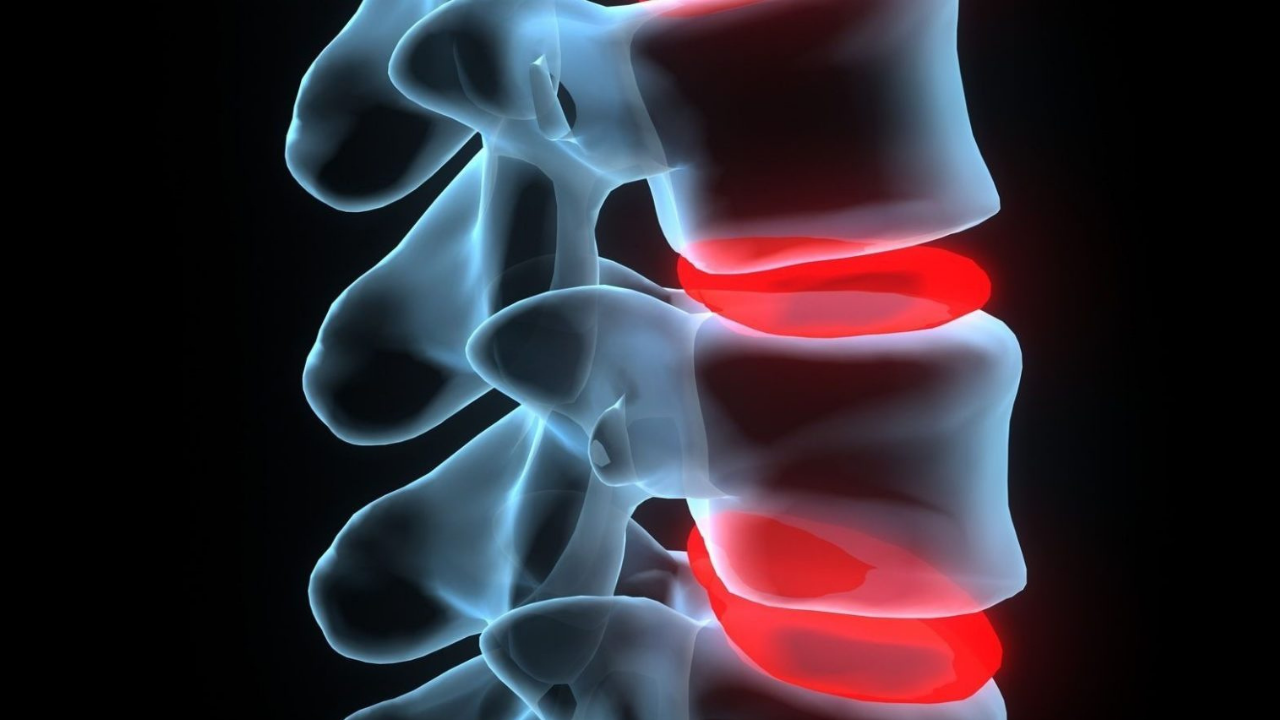
The spine is not just a stack of bones. Between each vertebra sits an intervertebral disc providing cushioning and flexibility, and at the back of each spinal segment sit two small joints — the facet joints (also called zygapophysial joints) — that guide and control the direction of spinal movement.
Like all joints, facet joints are lined with articular cartilage and surrounded by a synovial capsule that produces lubricating fluid. And like all joints, they are subject to wear, degeneration, inflammation, and arthritic change over time.
When facet joints degenerate or become inflamed, the result is facet joint syndrome — a condition characterized by:
- Deep, aching pain localized to the lower back, mid-back, or neck depending on affected level
- Pain that worsens with spinal extension (leaning back), rotation, or prolonged standing
- Morning stiffness that gradually improves with movement
- Referred pain into the buttocks, hips, or thighs (lumbar facet involvement) or into the shoulders and arms (cervical facet involvement)
- Pain that eases when sitting or leaning forward slightly
It is frequently misdiagnosed or lumped into the generic category of "nonspecific low back pain" — which is part of why so many patients spend years cycling through treatments that target the wrong structure.
Why Standard Treatments Reach Their Limits
The conventional management ladder for facet syndrome climbs predictably: NSAIDs and muscle relaxants first, then corticosteroid injections into the facet joint, then medial branch nerve blocks, then radiofrequency ablation (RFA) to burn the nerves carrying the pain signal.
Each rung has its place. Corticosteroid injections can provide meaningful relief — but that relief is, almost by definition, temporary. The injection suppresses inflammation without addressing the cartilage loss or joint degeneration driving it. Months later, the pain returns, and the patient is back for another injection.
Radiofrequency ablation can be more durable — silencing the pain signal for months to a year or more — but it's just that: silencing a signal. The underlying joint continues to degenerate. The nerves eventually regenerate, the pain returns, and repeat procedures carry increasing complexity.
Surgery — spinal fusion — is reserved for the most severe structural cases. It's a major intervention with a substantial recovery burden, and it permanently eliminates motion at the fused segment while increasing mechanical stress on adjacent levels.
What none of these approaches offer is regeneration. The ability to rebuild the cartilage, quiet the chronic inflammation at its source, and restore the joint's structural integrity. That's precisely the gap that stem cell therapy is designed to fill.
The Regenerative Approach: How Stem Cells Target Facet Joints
Facet joint cartilage, like cartilage elsewhere in the body, has a notoriously poor capacity for self-repair. It has limited blood supply, few resident repair cells, and when it degenerates, the body's natural healing response is insufficient to restore it. Left untreated, degeneration progresses.
Mesenchymal stem cells (MSCs) change this equation in three important ways.
Cartilage regeneration
MSCs are multipotent — they can differentiate into chondrocytes, the cells that produce and maintain cartilage matrix. When injected into a degenerated facet joint, they can contribute to the rebuilding of articular cartilage, restoring the joint surface that years of wear have eroded. This is not a cosmetic fix; it is structural repair at the cellular level.
Inflammation resolution
Chronic facet joint pain is driven in part by persistent low-grade inflammation — elevated levels of cytokines like IL-1β and TNF-α that perpetuate tissue breakdown and sensitize local pain receptors. MSCs are powerful immunomodulators. They actively suppress these pro-inflammatory signals and promote the shift toward a healing, regenerative environment — addressing the inflammatory component of pain directly rather than suppressing it pharmacologically.
Paracrine signaling
Beyond what they become, MSCs matter enormously for what they secrete. Through paracrine signaling — the release of growth factors, exosomes, and bioactive molecules — injected stem cells recruit the joint's own resident cells into the repair process. The effect is amplified: a relatively small number of introduced cells can trigger a substantially larger healing response than they could produce alone.
What the Clinical Evidence Shows
The research on stem cell therapy for facet syndrome has moved from theoretical models to direct human data — and the results are consistently encouraging.
The Munich Long-Term Study — Adipose-Derived Regenerative Cells (ADRCs)
A study published in the Journal of Personalized Medicine (2023) followed 37 patients with confirmed facet joint syndrome — all of whom had failed standard treatment for over a year — who received a single injection of autologous adipose tissue-derived regenerative cells (ADRCs). Cells were harvested from a small amount of the patient's own abdominal fat, processed using a CE-certified system, and injected under fluoroscopic guidance into the periarticular tissue of the affected facet joints. Every single patient reported improved pain scores at one week, one year, and five years post-treatment compared to baseline. The researchers concluded that long-term quality of life improvement was achievable with a single, minimally invasive session.
BM-MSC Extracellular Vesicles — Pilot Safety and Efficacy Study
A 2024 study published in Regenerative Medicine evaluated a novel approach: injecting bone marrow-derived MSC extracellular vesicles — nanoscale particles carrying the regenerative signaling cargo of stem cells — directly into the lumbar facet joint space of 20 patients with chronic low back pain. At three months, no adverse effects or complications were recorded. Average severity index scores improved by 65%, interference index scores by 72%, and Oswestry Disability Index scores by 58% — all statistically significant. The researchers described the therapy as "safe and promising" for facet-mediated low back pain.
The CellKine Trial — Mayo Clinic Phase 1
Mayo Clinic launched the CellKine trial to evaluate allogeneic, culture-expanded bone marrow-derived MSCs injected into lumbar facet joints in patients with painful facet arthropathy. The Phase 1 results, published in 2024, established safety and feasibility for this approach. Mayo has since progressed to a Phase 2 double-blind, randomized, crossover study examining efficacy — a rigorous design that reflects the growing scientific seriousness with which this treatment is being studied.
The Procedure: From Consultation to Recovery
Stem cell therapy for facet syndrome is performed on an outpatient basis. Here is what the process typically looks like:
Step 1 — Diagnostic Confirmation Before treatment, facet joint syndrome must be properly confirmed as the pain source. This typically involves clinical examination, MRI review, and in many cases a diagnostic medial branch block — a small injection of local anesthetic that temporarily numbs the facet joint nerve. If the patient experiences significant temporary pain relief from the block, it confirms the facet joint as the pain generator and establishes candidacy.
Step 2 — Cell Harvest For autologous procedures, cells are harvested from the patient's own adipose tissue (most commonly from the abdomen) via a minimally invasive lipoaspiration under local anesthesia. Bone marrow aspiration from the iliac crest is used in some protocols. For allogeneic treatments, donor-derived MSCs are used.
Step 3 — Cell Processing Harvested tissue is processed — either at point-of-care using a certified device or in a laboratory — to isolate, concentrate, and prepare the MSC fraction for injection.
Step 4 — Guided Injection Cells are delivered into the affected facet joint or periarticular space under fluoroscopic or ultrasound guidance. Precision is critical: accurate delivery ensures the cells reach the target tissue and aren't dispersed into surrounding structures.
Step 5 — Recovery and Follow-Up Most patients go home the same day. A period of reduced physical activity — typically several days to a week — is recommended. Pain may temporarily increase slightly in the first one to two weeks as the local environment responds to treatment; this is normal and resolves. Meaningful improvement typically begins at four to eight weeks, with continued progress through three to six months.
Who Should Consider This Treatment?
Stem cell therapy for facet syndrome is most appropriate for patients who:
- Have a confirmed diagnosis of facet joint syndrome or lumbar facet arthropathy
- Have experienced inadequate or short-lived relief from corticosteroid injections or nerve blocks
- Are seeking an alternative to radiofrequency ablation or spinal fusion
- Have chronic symptoms lasting more than six months
- Are in adequate general health to undergo a minor outpatient procedure
It is not appropriate for patients with active spinal infection, certain autoimmune conditions that affect treatment response, or those whose back pain originates from a different structural source — which is why accurate diagnosis before treatment is non-negotiable.
Frequently Asked Questions
How long do the results of stem cell therapy for facet syndrome last? Based on available data — including the five-year follow-up in the Munich ADRC study — improvements in pain and function can be durable over the long term. Individual outcomes vary based on age, disease severity, and lifestyle factors including activity level and body weight.
Is the procedure painful? The harvest procedure and injection are performed under local anesthesia and are well-tolerated by most patients. A temporary increase in soreness at the injection site in the days following treatment is common and typically mild.
How many sessions are needed? Many patients benefit from a single treatment session. Some cases — particularly more advanced degeneration — may benefit from a follow-up session at six to twelve months. Your specialist will advise based on your individual assessment.
Can stem cell therapy be combined with other treatments? Yes. It pairs particularly well with structured physical rehabilitation, which helps reinforce the mechanical improvements enabled by tissue repair. Some protocols also combine it with PRP (platelet-rich plasma) to enhance the regenerative environment.
Is this covered by insurance? Stem cell therapy for facet syndrome is generally not covered by standard insurance plans in most countries, as it remains in the clinical development phase. Your consultation team can provide full transparency on costs and what to expect.
What if my pain comes from multiple spinal levels? Multi-level facet syndrome can be addressed — injections can be performed at more than one level in the same session. The extent of treatment will be determined during your evaluation based on imaging and clinical findings.
Take the Next Step
Chronic facet joint pain is not something you simply have to endure. If standard treatments have offered only temporary relief, or if you're facing the prospect of nerve ablation or surgery, stem cell therapy may represent a meaningful and lasting alternative — one that works with your biology rather than around it.
Our specialists will review your imaging, evaluate your history, and give you an honest, personalized assessment of whether regenerative treatment is right for your case.
Book your consultation today.
This article is for informational purposes only and does not constitute medical advice. Diagnosis and treatment decisions should always be made in consultation with a qualified medical professional.
Quick Question